

























































-
rbutler708Asked on February 6, 2018 at 5:19 AM
Hi,
I have completed the following:
https://www.jotform.com/help/305-How-to-Show-Headers-and-Text-in-the-PDF
https://www.jotform.com/help/26-Setting-up-an-Autoresponder-Email to no avail.
I have enabled "Show Headers and Texts" in the Submission view, and I have created an Autoresponder per your instructions.
It has not worked. Item A is a Test send of the autoreply email. It is unacceptable because the email does not include Header and Texts or the PDF copy of their signed agreement.
Item A (below):
(TEST) WI Consent Form
Reply
|Today, 3:34 AMrbutler708@gmail.com{pdf-link}

{form_title} Name {name62} Name {name63} Name {name64} Name {name65} Name {name66} Name {name67} Name {name68} Lost Lab Forms {lostLab} Initial {clickTo} Sign with Full Name acknowledging Acceptance of Contract terms: {clickTo19} Sign with Full Name acknowledging Acceptance of Contract terms: {clickTo16} Initial Acknowledgement {initialAcknowledgement} Sign with Full Name acknowledging Acceptance of Contract terms: {clickTo25} Sign with Full Name acknowledging Acceptance of Contract terms: {clickTo34} Sign with Full Name acknowledging Acceptance of terms: {clickTo37} Full Name {fullName41} Date {date} Signature {signature45} Name {name} Item B (below): Below is item B. It represents what clients expect to receive via Autoresponder. Also, upon completing test submission, at no point was an email requested of the client to which the email would be sent. Thus our 2 questions are:
How do we send a copy of the complete PDF (as shown below with header and texts) via autoresponse?
How do we ensure a guest email is entered that they may receive an autoresponse that includes the completed PDF?
Please note the instructions in the links above failed to/did achieve the requested results.
Thanks
2018-01-25 10:16:12Patient Policies and ProceduresPreparing for your visits to Wellness IntegrativeWELLNESS INTEGRATIVE MEDICINE, INC.
We are a private member only Holistic practice which includes Holistic Family Medicine, Acupuncture, Massage, Yoga, Weight Loss, Nutrition planning, as well as Anti- Aging Medicine, including Complexion Blending. Cost of membership is $79/annually.
We accept Medicare, Blue Cross Blue Shield, Humana, UnitedHealth, and Cigna PPO. We are not enrolled in any HMO, ACO, or Medicaid programs as we are an independent Holistic practice. We offer discounted medicare rates to uninsured or underinsured individuals.
Be sure to bring your photo identification and a hard copy of your insurance card for scanning.
Scheduling & Portal Use:
Unlike corporate offices where doctors are scheduled to see over 24 patients in less 7 hours, with unlimited interruptions including unscheduled walk-ins, late patients, and phonecalls (which results in the typical 7-10 minuted rushed medical visit), our visits are 20, 40, or 60 minutes- uninterrupted and BY APPOINTMENT ONLY. Your visit will NOT be interrupted by phone calls or walk ins. You'll self check in from the comfort of your own home, and upon arrival immediately begin your medical visit. Your initial visit is 60 minute intake visit, and within 1 week, upon the return of the custom labs ordered during your intake process, we will complete your Annual Exam. We do require our own lab work based on our customized intake, and cannot use outside labs for this visit.
After these two initial visits (the mandated Intake, and one week later the Complete exam), you'll be scheduled for your complete exams annually (labs first) and thereafter, we will see you during regular office hours for your medical needs including urinary tract infections, sore throats, etc.
If there are medications for any chronic conditions, we will need to see you at least every 6 months to monitor for labs and side affects before further refills can be provided. We may provide a 30 day refill to help you continue your medications until that follow up appointment, but no further refills will be granted thereafter if you fail to follow up.
We ask that you do YOUR part in maintaining high quality visits for all, by scheduling your appointments and posting medical questions via portal. In the event you're running late, please feel free to leave a message by phone. It will be converted and submitted by email. If your call requires a response, we'll send word on the portal as to not delay another patient's visit. Messages submitted by portal will be responded to in less than 72 hours- most typically 6 hours, workload permitting.
We offer a "Portal Opt Out/Telephone Preferred" option for an additional $299.00 annual fee. This fee is added to your account after 3 telephone over portal opt outs such as lab request callins, physician callback requests. Scheduling call-ins are not considered not considered Portal Opt-Outs.
No Show visits incur a $30 fee.
Drop-Ins are disruptive to scheduled private patients and are not allowed
1. I agree to use the patient portal for non emergeny communications directly with my doctor or practice staff. I recognize that patients' portal communications take precidence over telephone calls/emails which frequently include solicitations and other time consuming distractions that adversely affect my doctor's ability to honor 20, 40, or 60 minute quality appointment times.
I acknowledge that Drop In visits are disruptive to scheduled patients and agree to use my portal access to avoid disruption. I acknowledge that disrespecting another patient's scheduled appointment with a Drop In visit in may be grounds for my dismissal from the practice.
Name
Tonya Conditt2. For after hour urgencies, I recognize to use an area Urgent Care (Advocate Olympia Fields and Ingalls are ok. We are not fans of St James Hosptial quality ratings. We'd like to also note the higher cost of Ingalls Urgent Aid).
Name
Tonya Conditt3. I agree to call 911 or go to the nearest ER for life- threatening emergencies. If I sustain a non- life threatening injury after hours (burn, sprain, laceration, infection, etc), I acknowledge that I should visit the Urgent Care/Quick Care center of my choice and follow up with my doctor within 3 days as needed.
Name
Tonya Conditt4. I recognize the importance of 'knowing my insurance coverage' (deductible, copay and/or co-insurance) in advance of my visits, and agree to report any changes to my insurance to Wellness in a timely fashion.
Name
Tonya Conditt5. I am not enrolled in any HMO program. If it is later determined that I do have HMO as my primary coverage, I acknowledge that I am responsible for payment of my bill in full. Further, I acknowledge that Wellness Integrative Medicine, Inc is NOT contracted with any HMO carriers and that if I have an HMO as a primary insurance, Wellness will NOT submit billing to any HMO. I will be responsible for the full charge as the secondary insurance will not be billed in leiu of billing your HMO.
Name
Tonya CondittHealing Medical Home/No Jerk Policy
In an age where the corporate medical models can make patients feel like a number and staff (who are often sick patients themselves) feel abused by administrators and patients alike, we understand that kindness heals and hostility does not (ie stress, hypertension, heart attack, etc). We maintain an affirming and supportive environment for both staff and patients at all times. Uncivil behavior is not tolerated.
We are committed to maintaining a Safe and Healing Medical Home for all. On behalf of both patients and staff, we stand in Respect, Sincerity, and Kindness. Whether in person or by phone, please be considerate of all staff and other patients, as they are expected to be considerate of you.
Name
Tonya CondittPractice Patient Collective Pay Program (Medical Co-Op)
Patients facing financial hardships are invited to participate in our medical co-operative: in exchange for medical savings, co-op members serve with our management team to defray general overhead costs. In the event of financial hardship, arrangements can be made by contacting our billing team via portal.
Name
Tonya CondittFinancial PolicyPayment Policy Effective 9/21/13
Thank you for choosing us as your medical home. We are committed to providing you with quality care at affordable prices in an environment you appreciate. Because there have been questions regarding insurance and payment responsibility for services rendered, we provide our payment policy. Please read it, and ask any questions you may have. A signed copy will be included in your chart.
1. Insurance. We are a hybrid model. We are a direct pay office but do accept some insurance, including Medicare. If you are not insured or are under insured, payment in FULL is required at the time of service. If you do not have an up to date insurance card, payment in full for each visit is required until your insurance is verified. Knowing your insurance benefits is your responsibility. Please contact your insurance company with any questions you may have regarding your coverage. We do offer payment plans for hardships. These are not an obligation on our part, but a courtesy. Please discuss this option with our receptionist and billing team.
2. Co- payments and deductibles. All copayments and deductibles must be paid at the time of service. This arrangement is part of your contract with your insurance company. Failure on my part to collect copayments and deductibles from patients can be considered fraud. Please help us in upholding the law by paying your co- payment at each visit.
3. Non-covered Services. Please be aware that some- and perhaps all- the services you receive may not be covered or are not considered ‘reasonable or necessary’ by Medicare or other insurers. These non covered services include completion of forms ($25), missed appointment charges ($30), returned check fee ($35), after hours/unscheduled weekend charges. You must pay for these services in FULL at the time of visit/request.
4. Proof of Insurance. All patients must complete our patient information forms before the visit. We will obtain a copy of your driver’s license and current valid insurance card to verify your insurance. If the correct insurance information is not provided in a timely manner, you will be responsible for the claim in its entirety.
5. Claims Submission. We will bill your insurance company. Your insurance company may need you to supply certain information directly. It is your responsibility to comply with their request. Please be aware that the balance of your claim is your responsibility whether or not your insurance company pays your claim. Your insurance benefit is a contract between you and your insurance company. Our office is not party to that contract.
6. Coverage Changes. If your insurance changes, please notify us before your next visit sot he appropriate changes can be made to help you receive your maximum benefits. If your insurance company does not pay your claim, the balance will automatically be billed to you.
7. Nonpayment. Please be aware that if a balance remains unpaid, you may be referred to collections agency and you and your immediate family members can be discharged from the practice. If this is to occur, you will be notified by certified mail that you have 30 days to find alternative medical care. During that 30 day period, we will be able to treat you on emergency basis only.
8. Payment Plans and Options. If you are experiencing financial hardship, please consider enrolled in one of our convenient payment plans. We will consider slide scale payment programs under certain situations such as student status, length of time you have been enrolled in our office, availability of other services appropriate for your needs.
9. Missed appointments. Our policy is to charge for missed appointments not canceled within a reasonable amount of time. The charge will be $30.00 per missed appointment. These charges will be your responsibility and billed directly to you. Please help us serve you and other patients by keeping your regularly scheduled appointment.
10. Routine physical (annual/comprehensive exam) versus chronic care. Some patients come for a physical and discussion of routine/chronic medical problems on the same day. A preventative service is also known as annual/comprehensive physical or exam. This includes age/gender appropriate history and physical exam, counseling, guidance, risk factor reduction, discussion of appropriate vaccinations and discussion/ordering of screening tests. If you would like to discuss any other medical problem (chronic or new) on the day you are in for a physical, a second charge will be billed to you or your insurance company. This is called an E/M or evaluation and management charge. If your insurance company does not allow the second charge, you will be responsible and it will be billed directly to you. To bypass this problem, we highly suggest that you come for your annual exam and medical visit separately.
11. After hours care. We offer standard early morning and evening hours twice weekly, and on Saturday per month. If a visit is needed after hours, we encourage you to visit the Urgent Care of your choice. If you choose a time outside of regular office hours, an additional concierger charge will be billed for after hours care. These late or weekend appointments are provided as a convenience to you. If your insurance does not cover this charge, it will be billed to you directly.
We are committed to providing the best treatment to you. Our prices are representative of the usual and customary charges for our area, and our services are unparalleled. Let us know if you have any questions.
I have read and understand the payment policy and agree to abide by its guidelines as indicated by my signature below.
Financial Policy
Wellness Integrative Med is here to help you in all aspects of your medical care, including financial arrangements. We offer a variety of alternatives for affordable quality medical healthcare coverage. You are, however, personally responsible for the payment of all medical services furnished to you and/or your dependents. This includes, but is not limited to, all uncovered tests, as well as all procedures performed for you in this office (Emergency and Non-Emergency).
If you have medical insurance, we will submit your insurance forms for payment from your insurance company and will credit such collections to your account. Any insurance co-payments are due and payable at the time of service.
If you do not have medical insurance, payment in full is expected to be made at the time services are rendered, unless special arrangements are made in advance. This office will bill you for the remaining portion of your balance, if any, once all insurance claims and payments have been received.
If you fail to pay your balance within 30 days after the statement was sent, we may assess a service charge of 1.5% of the remaining balance. If you do not make payments after 3 months of billing, your account may be sent to Collections. You agree to pay all collection costs incurred, in an amount not to exceed fifty percent (50%) of the unpaid balance, should any unpaid balance be referred to a collection agency. In addition should any unpaid balance be referred to an attorney for litigation, all reasonable attorney fees and court costs shall be paid for by you as allowed by the court.
A $35.00 service charge will be assessed on all Returned Checks. This office tries its best to estimate what services your insurance company will cover, but we cannot guarantee that your insurance will pay for all services.
It is your responsibility to know what services and benefits your medical insurance will cover. If it is determined that you are not eligible for coverage, you will be responsible for payment of all services provided.
Participating Insurance Companies include:
o Blue Cross Blue Shield PPO
o Cigna PPO
o Humana Health PPO
o United Health PPO
o Medicare
Patients must provide proof of insurance prior to treatment or be considered self-pay in which case, a credit or debit card will be required for monthly payment plan.
It is your responsibility to know what services and benefits your medical insurance will cover. If it is determined that you are not eligible for coverage, you will be responsible for payment of all services provided.
Please acknowledge the following. Your initials and signature represents your acceptance of our payment policy.
Initial
tcFORMS TELEPHONE CALLS AND NON COVERED SERVICES ("NCS")Please note that it is our policy to charge for forms completion as well as patient initiated sick calls that require the physician's exclusive medical time with patients. Be aware that some – and perhaps all – of the services you receive may not be covered or not considered reasonable or necessary by Medicare or other insurers.
You must pay for these particular services in FULL at the time of service. Examples of non covered services are:
Missed appointment charges ($30),
Returned check fee ($35),
Completion of forms (if not presented at the time of visit) ($20).
(Completion of forms includes letters written for you to your school, employer, lawyer, judge or anyone else).
In addition, statement fee ($15) if we have to bill you for your co-pay.
Please submit your co-pay at your appointment.
Records released at 75 cents per page . Per medical standards, with proper authorization, medical records transferred doctor to doctor a done with no charge.
Due to the unique nature of our practice, unlimited Telephone Telemed Services are offered exclusively to patients enrolled in our NCS, or Conceirge packages. Patients who wish to initiate telemed services for a new problem or concern to doctor are welcomed to do so as a fee for service. Telemed Services are available up to 15 minute increments:
up to 15 minutes: $30
15-30 minutes: $60
30 minutes plus: $90
*NCS Package: $349
*Concierge Package: $2500.00
*Weight Solutions $450
Any calls that our physicians may initiate to you will not be charged, as they will be considered an addendum to an already initiated visit as appropriate follow- up and/or outreach. Abnormal labs will not be posted to portal until appropriately discussed with our docs in person. If you would like to schedule a telemed visit or need to know if one is right for you, please discuss with our medical assistant or receptionists.
*for more information, visit: http://www.wellmedicalcenter.com/payments-fees/
Sign with Full Name acknowledging Acceptance of Contract terms:
Tonya CondittTonyaPolicies & Procedures for Using Wellness Integrative Med Patient Portal1. Read and familiarize yourself with these policies and procedures.
2. Read and sign the Informed Consent Page
3. Your registration will generate a user name and password.
4. Log on to the site and change your password.
5. Start using the site.
Available Components:
Messages: This allows you to send and receive secure e-mail from our office. This may include attachments, pictures, or other information. You can also ask for referrals, ask billing questions, or make suggestions as to how we can continue to improve our practice. DO NOT LEAVE URGENT MESSAGES HERE AS THERE IS A 48 HOUR TURN AROUND ON CALL PROCESSING!!
Lab/Test Results: This area allows you to receive copies of lab/test results which were done through any of our participating labs. You will also be able to see comments make by Dr. This is a read only area, but if you have any questions or concerns, you can use the messaging section to e-mail Dr Butler. These messages are reviewed typically within 48 hours.
Health Summary: This section allows you to view information entered into various parts of your electronic health record. These are available for you to review and check for accuracy as well as print for other physicians or to keep for your records. If things have changed or the record does not look complete, you can e-mail the office so we can update your record to make it as complete and up to date as possible.
Medications: Here you can see current and past medications that have been in your chart. You can also ask for refills through this part of the portal. Be sure to enter in the pharmacy you would like your prescriptions sent to!
Appointments: This section allows you to view upcoming appointments or even make appointments. We are rolling out the appointment section slowly to see how it works, so if there are no appointments slots available, call the office.
For any questions, please call us at 708.960.2986 or go to our website at www.wellmedicalcenter.com.
Informed Consent To Use Wellness Integrative Med, Inc Patient PortalPurpose of the Informed Consent Form
Wellness Integrative Med, Inc offers a secure way for you to view parts of your medical record and communicate with our staff. Secure messaging can be a valuable communication tool, but does have certain risks. In order to manage these risks, there are certain conditions of participation which have to be followed. This form’s intention is to show you have been informed of these risks and the conditions of participation and that you accept the risks and conditions of participation.
How to participate in the Patient Portal
The patient portal allows you to compose and receive e-mail, view parts of your chart, send refill requests and even schedule appointments. This is all done through a web site hosted by our electronic health record company. Once this form is agreed to and signed, you will be sent a welcome e-mail which will give you the user name and password necessary to sign in. Because of the security on the web site, all information passing between Wellness Integrative Med, Inc and you is encrypted so that it remains secure. Go to the web portal through our web site at www.wellmedicalcenter.com.
Protecting Your Private Health Information and Risks
This method of communication and viewing prevents unauthorized parties from being able to access or read messages while they are in transmission. However, the security of the messaging requires two additional things: the correct e-mail address and the correct person (or person authorized by that individual) getting access to the e-mail. These two factors are the responsibility of the patient. Please notify Wellness Integrative Med, Inc any time you change your e-mail address. You must also be very careful to keep track of who has access to your e-mail account so only you or someone designated by you can see the messages we send to you. If you have any concerns that someone else might have learned your password, go to the website and change it. We understand the importance of privacy in regards to your health care and will continue to strive to make all information as confidential as possible. We will never sell or give away any private information, including your e-mail address, without your written consent.
Conditions of Participation in the Portal
Access and participation in the Portal is totally optional and does not affect the care you will receive at Wellness Integrative Med, Inc. Therefore, we reserve the right to suspend or terminate this service at any time and for any reason. If we do terminate this service, we will notify you as promptly as possible. You also agree to not hold Wellness Integrative Med, Inc or any of its staff liable for any network infractions beyond its control. By signing below, you acknowledge that you have read the Policies and Procedures for the web portal and that you understand and comply with these.
NOTE: If you are 14 years of age or older, you may ask that your parents not be allowed to view your electronic medical records. If you do allow your parents/guardian to view your record, they may see information about any treatment you receive including information related to drug use or sexual activity. Please sign below if you give your parents the permission to view all your information. If you do NOT want this, please sign the opt out box below.
Sign with Full Name acknowledging Acceptance of Contract terms:
Tonya CondittTonyaPrescripition Refill and Other Frequently Asked QuestionsPRESCRIPTION REFILL POLICY
1. What's the deal with refills?
Refills are given at the time of your office visit and not in between visits. Your pharmacist can call for up to a 30 day refill, which we will approve only once the necessary follow up appointment has been made. When you are running low on your medication it is a reminder that you are probably due for an office visit. Dr Butler prescribes enough medication to last until your next office visit. The purpose of your appointment is to evaluate your medical problems to determine if you need a medication change, dosage change or even need the medicine anymore. If you are supposed to get blood work or other tests done, make sure you do this at least 10 days before your medicine runs out.
2. How much medication can I get at the time of my appointment?
If you have no issues and you are stable on your medication you can usually get a 90 day supply. Birth control medications will be refilled as 1 year given that they do not treat a condition but is considered preventative. If you have an ongoing medical issue that is stable you can often get a 3-6 month supply (high blood pressure pills, for example). If you have issues that are not under control then you usually need to return every 1-3 months for medication and evaluation (diabetes, for example). Some people who have dangerously out of control issues have to come back in 1-2 weeks. So the moral of the story is to get your health issues under control and make sure you ask for your refills at the time of your office visit so you are not surprised when the pharmacist says "Sorry, you have run out of medication."
3. Why can't I just call when I'm on my last pill like at other doctor's offices?
The average office is inundated with refill requests and hire lots of staff to handle the sheer volume of refill requests. This contributes to unaffordable healthcare costs, especially for other uninsured patients. Thirty percent of the phone calls to the average office are related to refill requests. Another 20% of calls are second calls in the same day from the same person who did not get their call returned. "It's 4:45 and nobody called me back! I just took my last pill! Help!" Please be efficient for all: schedule your follow up appointment before you are scheduled to run out of your medication.
4. Why is it my responsibility to keep track of my medication?
A physician usually has over 2500 patients to keep track of at the average office. We have approximately 400, a much smaller number to ensure personalized one on one care at a fair cost (thus minimal staff). Either way it is impossible for physicians to keep track of your medication refill dates. It is also hard on the pharmacists if you wait till the last minute to ask for a refill. Please keep track of your medication so you can ask in advance of using your last pill. It is best to schedule an appointment while you still have a week's supply left (especially if a holiday is coming up soon).
5. Anything else I can do to make things easier?
If you take a look at your prescriptions and try to get them renewed on the same cycle such as every 3,6,9 or 12 months then you will have them all in sequence and easy to remember the renewal date on all of them. Ask each time you go to the pharmacy to make sure you know when you will run out. Keep that list in your wallet so you will know when you come to your appointments.
6. What if I'm in a pinch? Are there exceptions?
Pharmacists will usually give you a 3-5 day supply to tide you over in an emergency. We make exceptions for situations in which you have had an emergency or are out of town.
7. I am sick. What about calling in antibiotics?
The only antibiotic Dr Butler will call in without a visit is one for a simple urinary tract infection (UTI) in a young woman who has a history of these. This is proven by research to be safe, effective and cost-effective. However, Dr Butler will not call in for someone who sounds very sick, or someone who has never had a UTI before. Any other infection requires a visit to determine if an antibiotic is appropriate.
Initial Acknowledgement
tcOther Frequently Asked QuestionsQ: Isn’t form completion or a 'work physicial' at any given time covered by my insurance?
A: No, your appointment covers E and M, evaluation and management of a problem. A "physical" covers discussion of prevention of medical problems, health maintenance, the physical itself and referral for age appropriate screening tests . Most insurance companies do not cover work physicals.
Q: Doctors used complete forms for me before for free. Why are they charging me now?
A: The health care environment is becoming more costly. Medical Malpractice insurance could go up anywhere from 10-25% this year. Also, Medicare’s reimbursement formula is flawed and scheduled to go down by 0.5% this year. And other insurances follow whatever Medicare does. Medicine is one of the few professions where the costs consistently increase far greater than inflation and the payment stays stagnant. Some docs are charging their patients membership fees in order to cover this. Some just increase the number of patients seen per day (and decrease the amount of time per visit to 10-15 minutes).
Q: Come on doc, it will take you only a minute!
A: If you need a physician to fill out the form, please note that it is not just a matter of a minute and some ink. It is our physician’s name, reputation and license on the line and there are costs associated with this.
Q: Are there any exceptions?
1) School and daycare forms for children (up to and including high school) if they have had a physical within the past year ( also not covered by your insurance, just a courtesy).
2) Disability forms when I have put you on disability. We cannot complete your disability form if your specialist or another provider has put you on disability.
3) Please have Preoperative clearance forms when you have come in for a preoperative physical. If you have not come in within 14 days before your surgery, a visit will be required or there
will be a charge.
4) EXAMPLES of forms that will be charged if presented AFTER your medical appointment (may not include all types of forms) :
• Handicapped parking permits
• Illness/Injury Insurance Forms
• Return to work form
• FMLA Family and Medical Leave Act
• College, Work, Camp physicals
• Immunization Form for school/work/other
• Boy scouts/Girl Scouts
• Insurance applications
• Adoption/Foster parent physical
• Prior Authorization for brand name drugs
• Authorization for Out of Plan Health Care
• Letters written on your behalf for your school, lawyer, judge, employer, application,
adoption, verifying health status or anything else.
Thank you very much for your understanding. It is only through enforcement of this policy that we can afford to give the kind of care you deserve: high quality care, same day/same week appointments, punctual appointments 30-60 minutes in length, online scheduling, email etc.
Sign with Full Name acknowledging Acceptance of Contract terms:
Tonya CondittTonyaASSIGNMENT OF BENEFITSFinancial Responsibility
All professional services rendered are charged to the patient and are due at the time of service, unless other arrangements have been made in advance with our business office. Necessary forms will be completed to file for insurance carrier payments.
Assignment of Benefits
I hereby assign all medical and surgical benefits, to include major medical benefits to which I am entitled. I hereby authorize and direct my insurance carrier(s), including Medicare, private insurance and any other health/medical plan, to issue payment check(s) directly to Wellness Integrative Medicine, Inc medical services rendered to myself and/or my dependents regardless of my insurance benefits, if any. I understand that I am responsible for any amount not covered by insurance.
Authorization to Release Information
I hereby authorize Wellness Integrative Medicine to: (1) release any information necessary to insurance carriers regarding my illness and treatments; (2) process insurance claims generated in the course of examination or treatment; and (3) allow a photocopy of my signature to be used to process insurance claims for the period of lifetime. This order will remain in effect until revoked by me in writing.
I have requested medical services from Wellness Integrative Medicien on behalf of myself and/or my dependents, and understand that by making this request, I become fully financially responsible for any and all charges incurred in the course of the treatment authorized.
I further understand that fees are due and payable on the date that services are rendered and agree to pay all such charges incurred in full immediately upon presentation of the appropriate statement. A photocopy of this assignment is to be considered as valid as the original.
Sign with Full Name acknowledging Acceptance of Contract terms:
Tonya CondittTonyaRelease of Billing InformationBy signing below I agree that all of the information I have provided is true and I give
permission to Wellness Integrative Medicine and it’s contracted associates permission to release medical records to my insurance company for the purpose of receiving payment. Under the circumstance that my insurance company does not pay for my scheduled office visits
I will be responsible for payment directly to my Physician, and/or Therapist. I acknowledge that services for fitness training, nutritional counseling, massage therapy, or esthetician services will not be billed to insurance and are my responsibility. Charges for those services are expected at the time of service or per membership agreement. I also acknowledge that in the event that I utilize multiple services under the Wellness Integrative umbrella, or am referred any medical specialist, my health records only as needed will be shared amongst the team as they collect to determine the best plannining for my overall well- being.
Sign with Full Name acknowledging Acceptance of terms:
Tonya CondittTonyaAcknowledgement of Receipt of the Notice of Protected Health InformationAcknowledgement of Receipt of the Notice of Protected Health Information
Wellness Integrative Medical,
18036 Gottschalk, Ave,
Homewood, IL 60430
708.960.2986
wellmedicalcenter.com
I have received a copy of the Notice of Privacy Practices regarding my Protected Health
Information (PHI) from Wellness Integrative Medical, Inc
Full Name
Tonya CondittDate
 Thursday, January 25, 2018
Thursday, January 25, 2018Signature

Name
Tonya Conditt -
AdrianReplied on February 6, 2018 at 7:00 AM
The Show Headers and Texts option will show headers and texts only in the PDF version of the submission and not in the email template.
If you want to edit the email template, please see the help article below:
How to Edit the Email Template for Notifications and Autoresponders
You can also send the PDF with the submission data attached to the email by turning ON the option to send the PDF Attachment in the advanced email settings.
Here is a cast:

I also suggest you reset the PDF design and try again.
To reset the PDF Design, go to your form's Submissions Page, click the PDF icon from the top menu then CUSTOMIZE PDF.
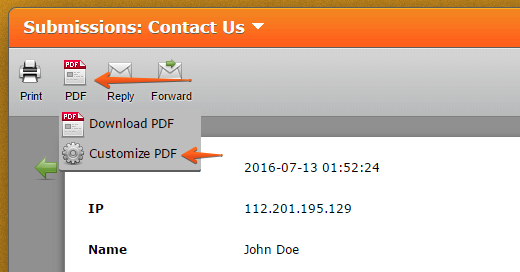
After that click the Reset button on the top right and save the changes.

Let us know if the issue persists.
- Templates
- Integrations
- INTEGRATIONS
- See 100+ integrations
- FEATURED INTEGRATIONS
 PayPal
PayPal- Slack
- Google Sheets
- Mailchimp
- Zoom
- Dropbox
- Google Calendar
- Hubspot
- Salesforce
- See more Integrations
- Products
- PRODUCTS
- Form Builder
- Jotform Enterprise
- Jotform Apps
- Store Builder
- Jotform Tables
- Jotform Inbox
- Jotform Mobile App
- Jotform Approvals
- Report Builder
- Smart PDF Forms
- PDF Editor
- Jotform Sign
- Jotform for Salesforce Discover Now
- Support



