Troy Intake Form

COVID-19 Vaccine Administration Record
Keep track of patient vaccination records online. More secure with GDPR, CCPA, and optional HIPAA compliance features. Download or print as PDFs. Free, easy-to-customize template.

Summer Camp Registration
Jotform’s Summer Camp Registration PDF Template is essential for camp coordinators looking for a better way to manage camper information. You can customize this sample to create the right enrollment form for future campers.
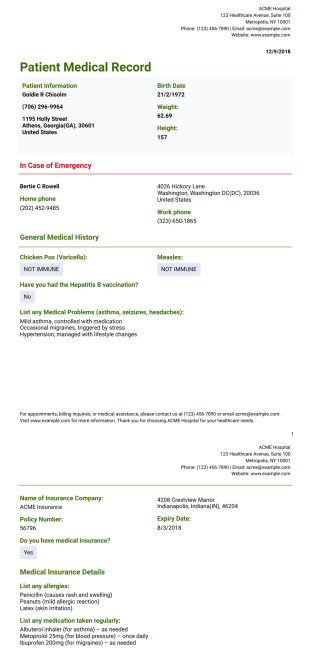
Patient Medical Record Template
Medical History Record PDF template lets you collect the patient's data such as personal information, contact information in an emergency case, general medical history. By using this sample, the doctor ensures the patient's better care and treatment.

Training Record Template
Keep track of employee training. Generate PDF training records automatically. Collect information and e-signatures. Easy to customize. No coding.

Vaccination Record Card
A vaccination record card is a crucial document used to document the details of vaccinations received by an individual

Portfolio Template
The Portfolio Template is a document used by freelance designers and job seekers to showcase their work to potential clients or employers