
Doctors have always recognized why data collection is so important in healthcare. But a lot about data collection has changed — the amount of it, the electronic health record (EHR) systems required to collect and manage it, and the constant vigilance necessary to comply with strict patient confidentiality laws.
Watch a really old episode of General Hospital, which first aired in 1963, and you’ll quickly see (besides very familiar plot lines) a clipboard hanging on a hook at the foot of every hospital bed. You’ll also see a doctor on his rounds (doctors were invariably male then), dramatically flipping through two or three pages on the clipboard to update himself on the patient’s condition. Those few pages were that fictional patient’s hospital records.
Real hospital records back then weren’t much longer. Keeping a record of treatment on paper was possible when a physician’s primary diagnostic tools were limited to stethoscopes, thermometers, X-ray machines, and rudimentary blood tests.
If you watch a contemporary TV show set in a hospital (or if you have the misfortune of needing treatment at the ER), you’ll see physicians ordering batteries of diagnostic tests and medical imaging while attaching heart rate and blood pressure monitors to a patient. And those procedures generate far more medical data than any clipboard can hold.
The long push for digital medical data
The shortcomings of paper medical records became pretty obvious in the 1990s as doctors started routinely using diagnostic imaging, a move that rapidly increased the sheer volume of data.
With each advancement in data technology, the medical field showed more interest in switching from paper files to digital medical records. It would be a monumental task, but everyone saw the potential benefits — physicians treating a patient could access electronic health records, which would vastly improve their ability to coordinate patient care and ultimately improve patient outcomes.
President George W. Bush took the first step forward when he established the Office of the National Coordinator for Health Information Technology in 2004. He gave the National Coordinator a mandate to promote the development and adoption of advanced information technology in health care, but that huge mandate came with a tiny budget.
And tiny budgets usually limit progress, which is exactly what happened for years — by 2008, just over 9 percent of U.S. hospitals had electronic health records.
Oddly enough, the Great Recession changed the fortunes of the initiative. When President Barack Obama was sworn into office in 2009, the nation was mired in the worst economic collapse since the Great Depression. Congress passed stimulus legislation, which included $30 billion to promote digital medical records, and the impact was dramatic.
According to a report by the Office of the National Coordinator for Health Information Technology, the percentage of acute care hospitals using electronic health records increased from 9.4 percent in 2008 to 83.8 percent in 2015.
The impact of HIPAA
Since the beginning of the internet, people have been as concerned about data privacy as they’ve been enthusiastic about data access. These same concerns exist for medical data systems. While the dream is to make all relevant information available to all professionals treating a patient, that dream has to function within the reality of stringent data protection mandates.
President Bill Clinton signed the Healthcare Insurance Portability and Accountability Act (HIPAA) into law on August 21, 1996. Among the many mandates in the law was a directive for the U.S. Department of Health and Human Services to write a Privacy Rule governing medical data collection, storage, and sharing.
The Privacy Rule defines Protected Health Information (PHI) broadly as “any information held by a covered entity which concerns health status, provision of healthcare, or payment for healthcare that can be linked to an individual.” The rule sets stiff penalties for compromising patient confidentiality — such as through a data breach or careless storage and handling that leaves patient data exposed, even if confidentiality isn’t compromised.
Every medical practice — from metropolitan hospitals to rural clinics and physicians in independent practice — relies on medical data to guide patient care (and to bill health insurance companies). But they also have to avoid even inadvertent HIPAA violations when it comes to that data.
Jotform is a turnkey, HIPAA-enabled solution for gathering, storing, and sharing PHI, and that begins with the first forms a patient fills out — patient intake forms.
Pro Tip
Use laboratory forms to collect test requests, patient details, and results in a consistent format. This can help healthcare teams keep records accurate, coordinate care more efficiently, and protect sensitive patient information.
The challenges that remain
There’s no dispute about why data collection is so important in healthcare — or about data collection practices being a burden on doctors.
Researchers from the University of New Mexico found that physicians spend two minutes filling out electronic health records for every one minute they spend with patients. The researchers concluded EHRs are the single largest cause of burnout — physicians have longer work days (because they’re completing EHRs) and less time to spend with family.
A survey of practicing physicians by Stanford Medicine in 2018 found that 59 percent of respondents said EHR systems should be revamped completely. In a 2017 open letter, the chief executives of 11 medical centers in the United States noted that electronic health records can enhance patient safety, but they warned that electronic recordkeeping had “radically altered and disrupted established workflows and patient interactions” for physicians and increased physician burnout.
The problems stem from the massive shift in EHR adoption — the 2009 stimulus legislation took the effort from lethargic to frantic in no time. Although the government implemented regulations in three phases, each phase only allowed EHR developers 18 months to incorporate new regulations into their products — and missing the deadlines meant not getting paid. So everyone adopted EHRs quickly, but the user experience got lost in the race to the finish line.
The search for solutions is on, and better technology will likely resolve the problems. One solution is dramatically improved speech-recognition software that’s capable of deciphering what physicians are saying — even in noisy settings like emergency rooms — and determining what information belongs where in the patient’s EHR.
In 2018, Allina Health in Minneapolis adopted the Dragon Medical One medical speech-recognition software from Nuance Communications. Alina has since seen improved clinician workflows, and its providers are generating 167 percent more documentation.
The switch from paper medical records to electronic records has been a steep challenge, and every solution has created new problems. But the systematic collection of patient data remains the greatest opportunity for improving treatment outcomes for individual patients — and medical care for everyone.
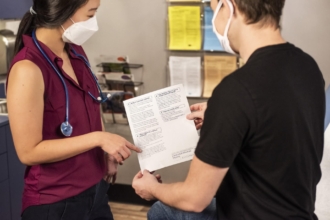
Photo by National Cancer Institute on Unsplash



























































































Send Comment: